Monitoring plaque and bleeding
Monitoring plaque biofilm and bleeding
Monitoring and recording plaque biofilm and bleeding levels enables the dental team to objectively assess the levels of plaque biofilm and gingival bleeding over time. In addition, if the patient is informed of their scores and understands what they mean, plaque and bleeding scores can be useful tools as part of motivation and behaviour change strategies. While a full mouth assessment is useful in specific circumstances, charting plaque and bleeding indices for index teeth on a more regular basis may be more practical.
Modified plaque biofilm and bleeding scores
The use of modified plaque biofilm and bleeding scores allows more rapid, objective assessment of oral hygiene and an indication of patient skill in oral hygiene and superficial gingival inflammation.
Both tools utilise Ramfjord’s Teeth, six index teeth (16, 21, 24, 36, 41, 44) that are distributed to best reflect the condition of the whole mouth. The scores can be communicated to the patient to aid in behaviour change strategies and they form an objective long-term assessment for the clinical team.
The plaque score relies on both the visual detection of plaque biofilm and detection using a probe at three sites on the index teeth (interproximal, buccal and palatal/lingual).
Visually assess the presence of plaque at three surfaces (interproximal, buccal and palatal/lingual) of the Ramfjord teeth. If no plaque is visible, use a probe to determine if plaque is present or absent.
- There are three possible scores for each surface:
2 = visible plaque without use of probe
1 = no visible plaque but a probe skimmed over the tooth surface reveals plaque
0 = no plaque - A percentage score for the index teeth is obtained by adding together the scores for each surface of the six Ramfjord teeth, dividing by 36 (i.e. the maximum plaque score possible) and multiplying the result by 100 as follows:
$$ \text{% score} = { \text{total score} \times 100 \over 36}$$
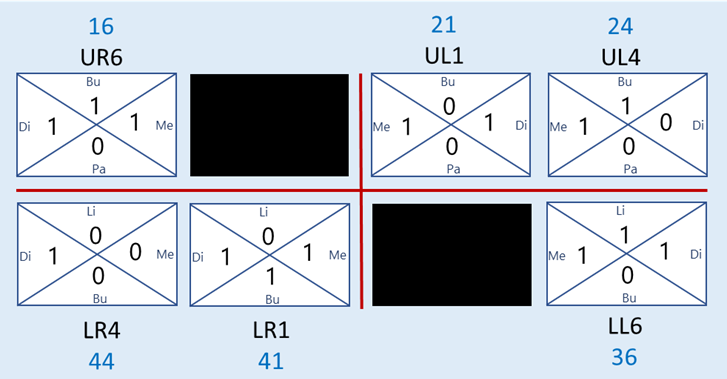
Calculating a modified plaque score

IP: interproximal; Bu: buccal; Pa: palatal; Li: lingual
Total score = 12
$$ \text{Plaque score} = { 12 \times 100 \over 36} = \text{33.33} = \text{33%}$$
Modified plaque score = 33%
A plaque score conversion table that can be used to quickly determine a modified plaque score from the index teeth score is available.
Modified bleeding score
The bleeding score measures bleeding from the gingival margin, rather than bleeding on probing from the base of the pocket. Bleeding from the gingival margin reflects how well the patient is able to carry out regular, effective plaque control, whilst bleeding on probing from the base of pockets indicates disease activity and periodontal breakdown.
Gently run a periodontal probe at 45 degrees around the gingival sulcus in a continuous sweep and visually monitor the presence or absence of bleeding at four sites (mesial, distal, buccal and palatal/lingual) for up to 30 seconds afterwards.
- There are two possible scores for each surface:
1 = bleeding present
0 = no bleeding - A percentage score for the index teeth is obtained by adding together the scores for each surface of the six Ramfjord teeth, dividing by 24 (i.e. the maximum bleeding score possible) and multiplying the result by 100 as follows:
$$ \text{% score} = { \text{total score} \times 100 \over 24}$$
Calculating a modified bleeding score
Di: distal; Bu: buccal; Me: Mesial; Pa: palatal; Li: lingual
Total score = 14
$$ \text{Bleeding score} = { 14 \times 100 \over 24} = \text{58.33} = \text{58%}.$$
Modified bleeding score = 58%
A bleeding score conversion table that can be used to quickly determine a modified plaque score from the index teeth score is available.
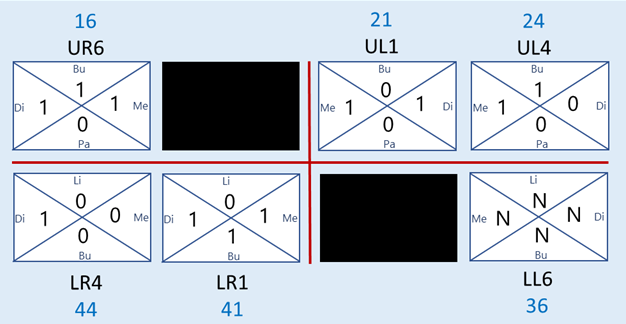
If a Ramfjord tooth is absent, an appropriate alternative tooth can be substituted (e.g. a second premolar substituted for a first premolar). If no appropriate tooth is available, for example if all lower left molars are missing, a code N should be assigned. The calculation of plaque and bleeding scores must be adjusted to take account of the missing teeth (e.g. where one code N is assigned, the maximum plaque score is reduced from 36 to 30 and the maximum bleeding score is reduced from 24 to 20).
Modified plaque score with missing teeth

Total score = 9
$$ \text{Modified plaque score} = { 9 \times 100 \over 30} = \text{30%}$$
Modified bleeding score with missing teeth
Total score = 11
$$ \text{Modified bleeding score} = { 11 \times 100 \over 20} = \text{55%}$$
Modified plaque score and modified bleeding score conversion tables are available.
The modified plaque and bleeding scores are an indication of patient’s skill in oral hygiene but these should not be used in isolation as indicators of patient engagement.* When considering which patients may benefit, or not, from more advanced treatment, a holistic assessment of patient engagement should consider other factors, such as patient attendance, level of oral hygiene knowledge/skill and patient wishes.
The BSP-S3 guideline6 includes a guide outlining the changes in plaque biofilm and bleeding scores which may indicate a favourable improvement in oral hygiene during Step 1 of therapy. These are:
- plaque levels of ≤20%, or ≥50% reduction in plaque from baseline measurements.
- marginal bleeding levels of ≤30%, or ≥50% reduction in marginal bleeding from baseline measurements.
Note that although some patients may engage to the best of their ability, they may not be able to achieve these levels of oral hygiene and plaque biofilm control due to factors such as manual dexterity or mental health problems. Whilst a 50% reduction in plaque or bleeding may indicate a favourable improvement, it might not be sufficient to achieve health and best treatment outcomes if the absolute percentage remains high. For instance a reduction from 80% to 40% plaque score is encouraging but for many patients with periodontitis will still impair treatment outcomes.
For patients who smoke, bleeding from the gingival margin and from the base of the periodontal pocket may be absent, even in the presence of periodontitis. Therefore, although bleeding scores can be recorded, they may not accurately reflect the clinical situation.
*Note that partial mouth recording systems tend to underestimate disease and that an abbreviated bleeding score obtained from index teeth may underestimate the true bleeding score that would be obtained from a full mouth assessment.
Full mouth plaque and bleeding assessment
A full mouth plaque biofilm and bleeding assessment can be performed as part of the full periodontal examination if additional information is needed about specific problem areas for plaque biofilm and inflammation control. This may also help the dental team to give their patient personalised oral hygiene instruction.
Assess the presence or absence of plaque biofilm (at four sites per tooth where full periodontal charting has been recorded) by running a probe gently around the tooth at the gingival margin. Score 1 if plaque biofilm is present and 0 if plaque biofilm is absent.
- A percentage score for the whole mouth is obtained by adding together the values for all teeth, dividing by the number of teeth and multiplying the result by 100 as follows:
$$ \text{% score} = { \text{number of surfaces with plaque} \times 100 \over \text{total number of teeth} \times 4}$$
After assessing plaque biofilm, observe each tooth at the four sites for the presence or absence of bleeding and calculate a percentage score for the whole mouth as follows:
$$ \text{% score} = { \text{number of surfaces with bleeding} \times 100 \over \text{total number of teeth} \times 4}$$
Plaque disclosing tablets or solutions can aid in the detection of plaque and act as a visual demonstration of plaque levels for patients.