Periodontal parameters
Bleeding on probing
In a full periodontal charting, bleeding from the base of the pocket is measured and indicates that active, progressive disease may be present. While measuring bleeding on probing, the specific presence and site of any suppuration on probing can also be recorded.
In non-smokers, an absence of bleeding on probing at any site suggests that active or progressing periodontal disease is absent. In people who smoke, the absence of bleeding on probing is not a reliable indicator that disease is not active or progressing.
Probing depth
Probing depth is the distance from the gingival margin to the base of the pocket (see figure: Periodontal pocket). The position of the gingival margin can change due to swelling or recession therefore probing depth measurement alone is not recommended for assessment of changes in periodontal support over time. However, changes in probing depth give a good indication of the response to periodontal treatment in the short term.
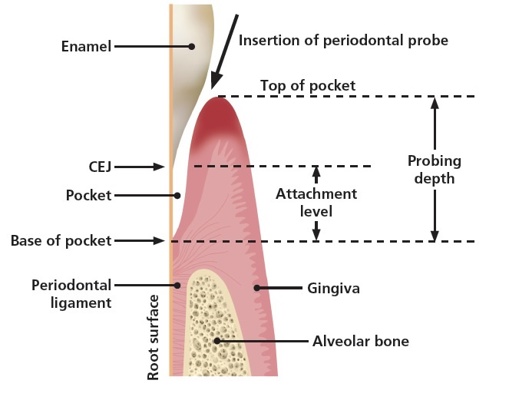
Simplified longitudinal section through a periodontal pocket.
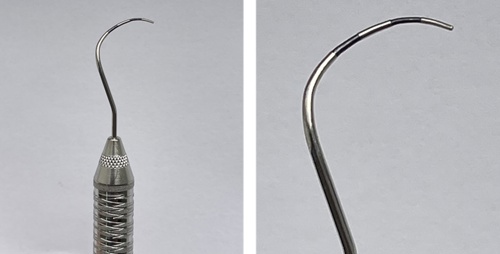
The probe should be inserted parallel to the root surface into the periodontal pocket and ‘walked’ around the gingival margin (see figure: Walking the probe). Probing depth should be measured at six sites per tooth.

A PCP 12 probe is ‘walked’ around the gingival margin of the tooth.
Measuring gingival recession
It can be difficult to accurately measure the position of the gingival margin in relation to the cementoenamel junction (CEJ) when the CEJ is not exposed. When measuring gingival recession (see figure: Measurement of recession), it is acceptable to record one measure of the greatest extent of gingival recession for both the buccal and lingual surfaces of the tooth.

The markings on the PCP 12 probe show that the recession is 2.5 mm.
Gingival margin position
The normal position of the gingival margin is coronal to the cementoenamel junction (CEJ; see figure: Periodontal pocket). Where the gingival margin is apical to the CEJ it is described as gingival recession. When recording the position of the gingival margin, indicate whether the margin is apical or coronal to the CEJ (i.e. if the patient has gingival hyperplasia or recession).
Clinical attachment loss
The clinical attachment level (CAL) combines the measurements of probing pocket depth and any gingival recession to give an overall indication of where the periodontal tissues attach to the root surface. It is measured from a fixed point, usually the CEJ, to the base of the periodontal pocket. This is considered the best measure of changes in residual periodontal support over time. If the CEJ is obscured, by for example a restoration margin, then another fixed reference point can be used to measure the relative clinical attachment loss. Most computerised clinical systems will calculate CAL automatically if measurements of probing pocket depth and recession are entered.
Measurement of furcation involvement
Damage from periodontitis can lead to furcation involvement of multi-rooted teeth. This can be measured using a furcation probe (see figure: Nabers furcation probe) and graded depending on the severity of the furcation involvement28 (see table: Grading of furcation involvement).
Grading of furcation involvement
| Grade | Description |
| 1 | Initial furcation involvement. The furcation opening can be felt on probing but the involvement is less than one third of the tooth width. |
| 2 | Partial furcation involvement. Loss of support exceeds one third of the tooth width but does not include the total width of the furcation. |
| 3 | Through-and-through involvement. The probe can pass through the entire furcation. |
Tooth mobility
Tooth mobility is assessed both horizontally and vertically. Horizontal mobility is measured by applying gentle pressure in a buccal-lingual direction, using two rigid instrument handles on either side of the tooth, and assessing the level of displacement (see figure: Tooth mobility). Vertical mobility is measured by applying gentle pressure on the crown of the tooth with a rigid instrument handle in a vertical direction.

Horizontal tooth mobility measured using two rigid instrument handles.
Mobility is graded as shown below.29
Grading of tooth mobility
| Grade | Description |
| 0 | ‘Physiological’ mobility measured at the crown level. |
| 1 | Increased mobility of the crown of the tooth to at the most 1 mm in a horizontal direction. |
| 2 | Increased mobility of the crown of the tooth exceeding 1 mm but less than 2 mm in a horizontal direction. |
| 3 | Mobility of the crown of the tooth in both horizontal and vertical directions. |